Dysembryoplastic neuroepithelial tumour
[1] These are glioneuronal tumours comprising both glial and neuron cells and often have ties to focal cortical dysplasia.
[2] Varying subclasses of DNTs have been presently identified, with dispute existing in the field on how to properly group these classes.
[4] With DNTs often causing epileptic seizures, surgical removal is a common treatment, providing high rates of success.
[1] Other findings suggest that DNTs require a reclassification to associate them with oligodendrogliomas, tumours that arise from solely glial cells.
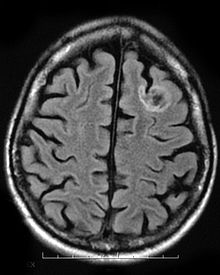
[3] A dysembryoplastic neuroepithelial tumour is commonly diagnosed in patients who are experiencing seizures with magnetic resonance imaging (MRI), electroencephalogram (EEG).
[4] Typical DNTs can be detected in an EEG scan when there are rapid repetitive spikes against a contrasted background.
For the tumor to be completely removed doctors need to perform resections consisting an anterior temporal lobectomy or amygdalo-hippocampectomy.
On the other hand, if resections are not performed, and the tumour is not completely removed, then the patient is still at risk of experiencing the seizures.
[4] In a study done by Bilginer et al., 2009, looking at patients whose tumour was not completely removed, and saw that they were still experiencing seizures, concluding that the incomplete resection as a being a failure.
[4] This evidence shows that surgery and complete resections are one of the better approaches in treating dysembryoplastic neuroepithelial tumours.
Furthermore, a longer period of epilepsy, and patients older in age are less likely to have a full recovery and remain seizure free.
[1] Few other neurological deficits are associated with DNTs, so that earlier detection of the tumour before seizure symptoms are rare.