Neurofibroma
Neurofibromas arise from nonmyelinating-type Schwann cells that exhibit biallelic inactivation of the NF1 gene that codes for the protein neurofibromin.
According to the World Health Organization classification system, dermal and plexiform neurofibromas are grade I tumors.
Three kinds are distinguished:[4] Dermal neurofibromas typically arise in the teenage years and are often associated with the onset of puberty.
In people with neurofibromatosis type I, they tend to continue to increase in number and size throughout adulthood, although limits exist as to how big they get, and cases progress at highly variable rates.
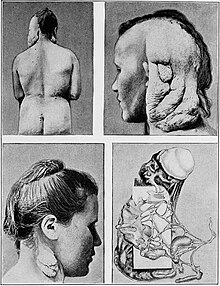
[citation needed] Plexiform neurofibromas have the potential to cause severe clinical complications if they occur in certain areas.
Loss of RAS control leads to increased activity of other signaling pathways including RAF, ERK1/2, PI3K, PAK and mTOR-S6 kinase.
Neurofibromin has other growth-regulatory properties besides its ability to regulate RAS activity, but these other functions are poorly understood at this time.
While myelinating Schwann cells cover large diameter (>1 micrometer) peripheral nervous system (PNS) axons with myelin, nonmyelinating Schwann cells encapsulate small diameter PNS axons with their cytoplasmic processes.
It is unknown at this time why, if both types of Schwann cells exhibit bilallelic inactivation of the NF1 gene, only the nonmyelinating variety give rise to neurofibromas.
While one defective allele may be inherited, loss of heterozygosity (LOH) must occur before a neurofibroma can form; this is called the 'two-hit hypothesis'.
[citation needed] Once a nonmyelinating Schwann cell has suffered inactivation of its NF1 genes, it begins to proliferate rapidly.
The mast cells then secrete mitogens or survival factors that alter the developing tumor microenvironment and result in neurofibroma formation.
[citation needed] Dermal and plexiform neurofibromas differ in later development stages, but the details are unclear at this point.
However, it is strongly advised that a test treatment be performed to judge the effectiveness of the procedure and whether the developed scar is an acceptable trade-off.
ACE inhibitors are currently used to treat hypertension and congestive heart failure, to avert remodeling and reinfarction after myocardial infarction, and to ameliorate diabetic nephropathy and other renal diseases.
ACE inhibitors work by indirectly down regulating TGF-beta, which is a growth factor that has been shown to influence the development of tumors.
[30] Early research has shown potential for using the c-kit tyrosine kinase blocking properties of imatinib to treat plexiform neurofibromas.