Sievert
The sievert (symbol: Sv[note 1]) is a unit in the International System of Units (SI) intended to represent the stochastic health risk of ionizing radiation, which is defined as the probability of causing radiation-induced cancer and genetic damage.
According to the International Commission on Radiological Protection (ICRP), one sievert results in a 5.5% probability of eventually developing fatal cancer based on the disputed linear no-threshold model of ionizing radiation exposure.
Conventionally, deterministic health effects due to acute tissue damage that is certain to happen, produced by high dose rates of radiation, are compared to the physical quantity absorbed dose measured by the unit gray (Gy).
[3] The SI definition given by the International Committee for Weights and Measures (CIPM) says: "The quantity dose equivalent H is the product of the absorbed dose D of ionizing radiation and the dimensionless factor Q (quality factor) defined as a function of linear energy transfer by the ICRU" The value of Q is not defined further by CIPM, but it requires the use of the relevant ICRU recommendations to provide this value.
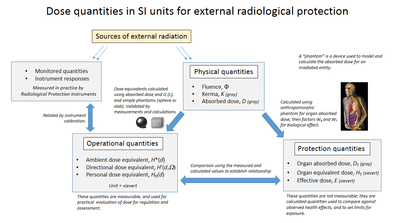
Consequently, this has required the creation of a number of different dose quantities within a coherent system developed by the ICRU working with the ICRP.
The ICRU is primarily responsible for the operational dose quantities, based upon the application of ionising radiation metrology, and the ICRP is primarily responsible for the protection quantities, based upon modelling of dose uptake and biological sensitivity of the human body.
However, there are joint ICRU/ICRP proposals to simplify this system by changes to the operational dose definitions to harmonise with those of protection quantities.
In this way they are used for practical dose control, by providing an estimate or upper limit for the value of the protection quantities related to an exposure.
[10] Simple (non-anthropomorphic) "phantoms" are used to relate operational quantities to measured free-air irradiation.
According to the ICRP, the ICRU "sphere phantom" in most cases adequately approximates the human body as regards the scattering and attenuation of penetrating radiation fields under consideration.
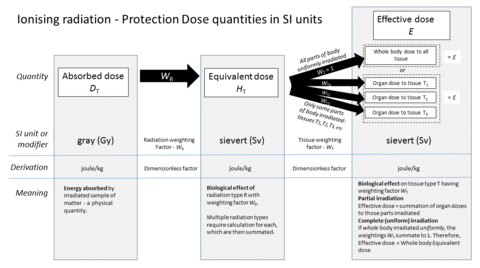
[14][15][13] These quantities cannot be measured in practice but their values are derived using models of external dose to internal organs of the human body, using anthropomorphic phantoms.
The calculation starts with organ absorbed dose, and then applies radiation and tissue weighting factors.
It is this biological component that is being expressed when using sieverts rather than the actual energy delivered by the incident absorbed radiation.
Some tissues like bone marrow are particularly sensitive to radiation, so they are given a weighting factor that is disproportionally large relative to the fraction of body mass they represent.
Other tissues like the hard bone surface are particularly insensitive to radiation and are assigned a disproportionally low weighting factor.
The operational quantities are used in practical applications for monitoring and investigating external exposure situations.
This means the radiation is equivalent to that found 10 mm within the ICRU sphere phantom in the direction of origin of the field.
This means the radiation is equivalent to that found at a depth of 0.07 mm in the ICRU sphere phantom.
For area monitoring of effective dose of whole body it would be: The driver for this is that H∗(10) is not a reasonable estimate of effective dose due to high energy photons, as a result of the extension of particle types and energy ranges to be considered in ICRP report 116.
[5] The ICRP further states "For internal exposure, committed effective doses are generally determined from an assessment of the intakes of radionuclides from bioassay measurements or other quantities (e.g., activity retained in the body or in daily excreta).
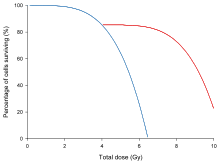
Deterministic (acute tissue effect) events happen with certainty, with the resulting health conditions occurring in every individual who received the same high dose.
Stochastic (cancer induction and genetic) events are inherently random, with most individuals in a group failing to ever exhibit any causal negative health effects after exposure, while an indeterministic random minority do, often with the resulting subtle negative health effects being observable only after large detailed epidemiology studies.
The consensus of nuclear regulators, governments and the UNSCEAR is that the incidence of cancers due to ionizing radiation can be modeled as increasing linearly with effective dose at a rate of 5.5% per sievert.
A model of deterministic risk would require different weighting factors (not yet established) than are used in the calculation of equivalent and effective dose.
[1] For comparison, natural radiation levels inside the United States Capitol are such that a human body would receive an additional dose rate of 0.85 mSv/a, close to the regulatory limit, because of the uranium content of the granite structure.
[31] According to the conservative ICRP model, someone who spent 20 years inside the capitol building would have an extra one in a thousand chance of getting cancer, over and above any other existing risk (calculated as: 20 a·0.85 mSv/a·0.001 Sv/mSv·5.5%/Sv ≈ 0.1%).
All conversions between hours and years have assumed continuous presence in a steady field, disregarding known fluctuations, intermittent exposure and radioactive decay.
Notes on examples: The sievert has its origin in the röntgen equivalent man (rem) which was derived from CGS units.
As with every SI unit named for a person, its symbol starts with an upper case letter (Sv), but when written in full, it follows the rules for capitalisation of a common noun; i.e., sievert becomes capitalised at the beginning of a sentence and in titles but is otherwise in lower case.
Regulatory limits and chronic doses are often given in units of mSv/a or Sv/a, where they are understood to represent an average over the entire year.