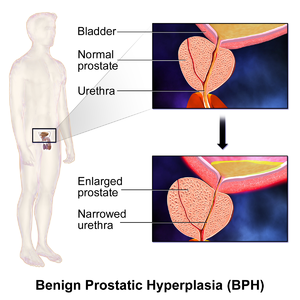
Benign prostatic hyperplasia
[1] Risk factors include a family history, obesity, type 2 diabetes, not enough exercise, and erectile dysfunction.
[2] The underlying mechanism involves the prostate pressing on the urethra thereby making it difficult to pass urine out of the bladder.
[2] Other herbal medicines somewhat effective at improving urine flow include beta-sitosterol[5] from Hypoxis rooperi (African star grass), pygeum (extracted from the bark of Prunus africana),[6] pumpkin seeds (Cucurbita pepo), and stinging nettle (Urtica dioica) root.
[21] Most experts consider androgens (testosterone and related hormones) to play a permissive role in the development of BPH.
The importance of DHT in causing nodular hyperplasia is supported by clinical observations in which an inhibitor of 5α-reductase such as finasteride is given to men with this condition.
[35] Studies looking for a correlation between prostatic hyperplasia and serum estrogen levels in humans have generally shown none.
[37] If confirmed, this mechanism explains why serum androgen levels do not seem to correlate with BPH and why giving exogenous testosterone would not make much difference.
Studies indicate that dietary patterns may affect the development of BPH, but further research is needed to clarify any important relationship.
Such misrepairs make the muscular tissue weak in functioning, and the fluid secreted by glands cannot be excreted completely.
Then, the accumulation of fluid in glands increases the resistance of muscular tissue during the movements of contractions and dilations, and more and more myofibers will be broken and replaced by collagen fibers.
(Carcinoma of the prostate typically occurs in the posterior lobe – hence the ability to discern an irregular outline per rectal examination).
The earliest microscopic signs of BPH usually begin between the age of 30 and 50 years old in the PUG, which is posterior to the proximal urethra.
[2] However, checking blood PSA levels for prostate cancer screening is controversial and not necessarily indicated in every evaluation for BPH.
[2] Notable causes of neurogenic bladder include disorders of the central nervous system such as Parkinson's disease, multiple sclerosis, and spinal cord injuries as well as disorders of the peripheral nervous system such as diabetes mellitus, vitamin B12 deficiency, and alcohol-induced nerve damage.
[2] Individuals affected by heart failure often experience nighttime awakenings to urinate due to redistribution of fluid accumulated in swollen legs.
[2] In contrast, calcium channel blockers and anticholinergic medications can worsen urinary retention by promoting bladder muscle relaxation.
[2] When treating and managing benign prostatic hyperplasia, the aim is to prevent complications related to the disease and improve or relieve symptoms.
Lifestyle alterations to address the symptoms of BPH include physical activity,[59] decreasing fluid intake before bedtime, moderating the consumption of alcohol and caffeine-containing products, and following a timed voiding schedule.
However, the quality of evidence was very low and therefore it remains uncertain whether physical activity is helpful in men experiencing urinary symptoms caused by benign prostatic hyperplasia.
[62] A meta-analysis found no differences between the standing and sitting positions for healthy males, but that, for elderly males with lower urinary tract symptoms, voiding in the sitting position-- [63] This urodynamic profile is associated with a lower risk of urologic complications, such as cystitis and bladder stones.
[71][58][72] Alpha blockers relax smooth muscle in the prostate and the bladder neck, thus decreasing the blockage of urine flow.
Common side effects of alpha-blockers include orthostatic hypotension (a head rush or dizzy spell when standing up or stretching), ejaculation changes, erectile dysfunction,[73] headaches, nasal congestion, and weakness.
For men with LUTS due to an enlarged prostate, the effects of naftopidil, tamsulosin, and silodosin on urinary symptoms and quality of life may be similar.
[74] Non-selective alpha-blockers such as terazosin and doxazosin may also require slow dose adjustments as they can lower blood pressure and cause syncope (fainting) if the response to the medication is too strong.
[76] When used together with alpha-blockers, no benefit was reported in short-term trials, but in a longer-term study (3–4 years) there was a greater reduction in BPH progression to acute urinary retention and surgery than with either agent alone, especially in people with more severe symptoms and larger prostates.
[83] A 2018 Cochrane review of studies on men over 60 with moderate to severe lower urinary tract symptoms analyzed the impacts of phosphodiesterase inhibitors (PDE) in comparison to other drugs.
The evidence in this review found that there is probably no difference between PDE and alpha blockers, however when used in combination they may provide a greater improvement in symptoms (with more side effects).
Several phosphodiesterase-5 inhibitors are also effective but may require multiple doses daily to maintain adequate urine flow.
[93] In 2011, the U.S. Food and Drug Administration approved tadalafil to treat the signs and symptoms of benign prostatic hyperplasia, and for the treatment of BPH and erectile dysfunction (ED), when the conditions occur simultaneously.
[164] Particularly, several reviews found that saw palmetto extract, while one of the most commonly used, is no better than a placebo both in symptom relief and in decreasing prostate size.