Rheumatic fever
[2] Signs and symptoms include fever, multiple painful joints, involuntary muscle movements, and occasionally a characteristic non-itchy rash known as erythema marginatum.
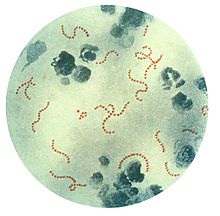
[1] Diagnosis of RF is often based on the presence of signs and symptoms in combination with evidence of a recent streptococcal infection.
[3] Treating people who have strep throat with antibiotics, such as penicillin, decreases the risk of developing rheumatic fever.
The similarity between antigens of Streptococcus pyogenes and multiple cardiac proteins can cause a life-threatening type II hypersensitivity reaction.
[citation needed] This inflammation occurs through direct attachment of complement and Fc receptor-mediated recruitment of neutrophils and macrophages.
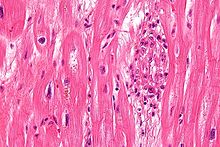
Characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy.
Involvement of the endocardium typically results in fibrinoid necrosis and wart formation along the lines of closure of the left-sided heart valves.
Warty projections arise from the deposition, while subendocardial lesions may induce irregular thickenings called MacCallum plaques.
[citation needed] Chronic rheumatic heart disease (RHD) is characterized by repeated inflammation with fibrinous repair.
[19] The majority of morbidity and mortality associated with rheumatic fever is caused by its destructive effects on cardiac valve tissue.
[18] The complicated pathogenesis of RHD is not fully understood, though it has been observed to use molecular mimicry via group A streptococci carbohydrates and genetic predisposition involving HLA Class II genes that trigger autoimmune reactions.
[21] This causes an autoimmune reaction against native tissues in the heart that are incorrectly recognized as "foreign" due to the cross-reactivity of antibodies generated as a result of epitope sharing.
[23] Self-antigen-specific antibodies generated via molecular mimicry between human proteins and streptococcal antigens up-regulate VCAM-1 after binding to the valvular endothelium.
The dominant contributors are a component of MHC class II molecules, found on lymphocytes and antigen-presenting cells, specifically the DR and DQ alleles on human chromosome 6.
[37][38][39] An April 2013 review article in the Indian Journal of Medical Research stated that echocardiographic and Doppler (E & D) studies, despite some reservations about their utility, have identified a massive burden of rheumatic heart disease, which suggests the inadequacy of the 1992 Jones' criteria.
[41] The last revision of 2015 suggested variable diagnostic criteria in low-risk and high-risk populations to avoid overdiagnosis in the first category and underdiagnosis in the last one.
[34] Minor criteria Rheumatic fever can be prevented by effectively and promptly treating strep throat with antibiotics.
[45] Antibiotic prophylaxis after an episode of acute rheumatic fever is recommended owing to the high likelihood of recurrence.
[citation needed] Monthly injections of long-acting penicillin must be given for a period of five years in patients having one attack of rheumatic fever.
Another important cornerstone in treating rheumatic fever includes the continual use of low-dose antibiotics (such as penicillin, sulfadiazine, or erythromycin) to prevent recurrence.
[52] However, due to side effects like gastritis and salicylate poisoning, necessitating serum monitoring of salicylate levels, and the risk of Reye syndrome, a serious and potentially deadly condition that may arise in children treated with aspirin or aspirin-containing products, alternatives to aspirin have been sought, especially in children.
[48] While evidence suggests that treatment of rheumatic fever–associated arthritis with naproxen may be equally effective as with aspirin,[48][53] its role in managing carditis has not been established.
[55] Corticosteroids may be considered, especially in people with allergies to NSAIDs or severe disease,[48] although use of steroids may cause tissue atrophy, which could present challenges during future cardiac surgery for valve repair.
This requires the usual treatment for heart failure: ACE inhibitors, diuretics, beta blockers, and digoxin.
[57] In Western countries, rheumatic fever has become fairly rare since the 1960s, probably due to the widespread use of antibiotics to treat streptococcus infections.
[59] Rheumatic fever primarily affects children between ages 5 and 17 years and occurs approximately 20 days after strep throat.
[citation needed] The rate of development of rheumatic fever in individuals with untreated strep infection is estimated to be 3%.
[citation needed] The recurrence of rheumatic fever is relatively common in the absence of maintenance of low dose antibiotics, especially during the first three to five years after the first episode.