Ground-glass opacity
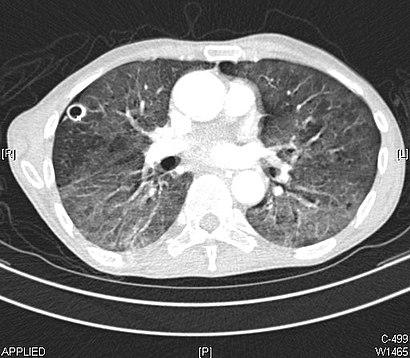
Ground-glass opacity (GGO) is a finding seen on chest x-ray (radiograph) or computed tomography (CT) imaging of the lungs.
It is typically defined as an area of hazy opacification (x-ray) or increased attenuation (CT) due to air displacement by fluid, airway collapse, fibrosis, or a neoplastic process.
[2][3] In both CT and chest radiographs, normal lungs appear dark due to the relative lower density of air compared to the surrounding tissues.
When air is replaced by another substance (e.g. fluid or fibrosis), the density of the area increases, causing the tissue to appear lighter or more grey.
In CT, the term refers to one or multiple areas of increased attenuation (density) without concealment of the pulmonary vasculature.
In chest radiographs, the term refers to one or multiple areas in which the normally darker-appearing (air-filled) lung appears more opaque, hazy, or cloudy.
Pneumocystis pneumonia, an infection typically seen in immunocompromised (e.g. patients with AIDS) or immunosuppressed individuals, is a classic cause of diffuse GGOs.
Benign conditions potentially leading to the formation of nodular GGOs include aspergillosis, acute eosinophilic pneumonia, focal interstitial fibrosis, granulomatosis with polyangiitis, IgA vasculitis, organizing pneumonia, pulmonary contusion, pulmonary cryptococcus, and thoracic endometriosis.
Focal interstitial fibrosis presents a unique challenge when differentiating from malignant nodular GGOs on CT imaging.
One large review study found that 80% of nodular GGOs which were present on repeated CT imaging represented either pre-malignant or malignant growths.
AAH is a pre-malignant cause of nodular GGO and is more commonly associated with lower attenuation on CT and smaller nodule size (<10 mm) compared to adenocarcinoma.
[9][10] Centrilobular GGOs refer to opacities occurring within one or multiple secondary lobules of the lung, which consist of a respiratory bronchiole, small pulmonary artery, and the surrounding tissue.
Important non-infectious causes include granulomatosis with polyangiitis, metastatic disease with pulmonary hemorrhage, and some types of idiopathic interstitial pneumonias.
[18] Several studies have described a pattern among initial, intermediate, and hospital discharge imaging findings in the disease course of COVID-19.
These patients may develop lung "white-out" with progression to acute respiratory distress syndrome (ARDS) requiring treatment escalation.
[22] The first usage of "ground-glass opacity" by a major radiological society occurred in a 1984 publication of the American Journal of Roentgenology.
[23] The original published definition read as: "Any extended, finely granular pattern of pulmonary opacity within which normal anatomic details are partly obscured; from a fancied resemblance to etched or abraded glass.