Supraventricular tachycardia
[2] The symptoms of SVT include palpitations, feeling of faintness, sweating, shortness of breath, and/or chest pain.
Stress, exercise, and emotion can all result in a normal or physiological increase in heart rate, but they can precipitate SVT in rare cases.
The rapid heart rate, if fast enough, reduces the opportunity for the "pump" to fill between beats decreasing cardiac output and consequently blood pressure.
An accessory "bypass tract" can avoid the AV node and its protection so that the fast rate may be directly transmitted to the ventricles.
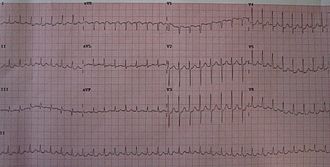
In the clinical setting, the distinction between narrow and wide complex tachycardia (supraventricular vs. ventricular) is fundamental since they are treated differently.
In the less common situation in which a wide-complex tachycardia may be supraventricular, a number of algorithms have been devised to assist in distinguishing between them.
[15] In general, a history of structural heart disease markedly increases the likelihood that the tachycardia is ventricular in origin.
This is a low-risk procedure that uses a catheter inside the heart to deliver radiofrequency energy to locate and destroy the abnormal electrical pathways.
[26] This therapy has further improved the treatment options for AVNRT (and other SVTs with pathways close to the AV node), widening the application of curative ablation to young patients with relatively mild but still troublesome symptoms who might not have accepted the risk of requiring a pacemaker.
Episodes can be treated when they occur by Valsalva maneuver, adenosine injection or taking a AV node blocking agent as pill-in-pocket, but regular medication may also be used to prevent or reduce recurrence.
[27] Lifestyle changes, medication and heart procedures may be needed to control or eliminate the rapid heartbeats and related symptoms.