Kidney stone disease
[2] If a stone grows to more than 5 millimeters (0.2 inches), it can cause blockage of the ureter, resulting in sharp and severe pain in the lower back that often radiates downward to the groin (renal colic).
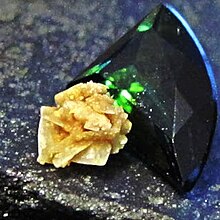
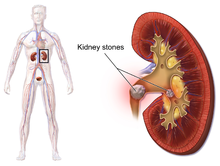
[2] Calculi are typically classified by their location: nephrolithiasis (in the kidney), ureterolithiasis (in the ureter), cystolithiasis (in the bladder), or by what they are made of (calcium oxalate, uric acid, struvite, cystine).
[7][9] Larger calculi may be helped to pass with the medication tamsulosin[10] or may require procedures such as extracorporeal shock wave lithotripsy, ureteroscopy, or percutaneous nephrolithotomy.
[2] Renal calculi have affected humans throughout history with a description of surgery to remove them dating from as early as 600 BC in ancient India by Sushruta.
In this context, epidemiological studies are striving to elucidate the worldwide changes in the patterns and the burden of the disease and identify modifiable risk factors that contribute to the development of renal calculi.
[15] Renal colic caused by kidney stones is commonly accompanied by urinary urgency, restlessness, hematuria, sweating, nausea, and vomiting.
[19] High dietary intake of animal protein,[14] sodium, sugars including honey, refined sugars, fructose and high fructose corn syrup,[20] and excessive consumption of fruit juices may increase the risk of kidney stone formation due to increased uric acid excretion and elevated urinary oxalate levels (whereas tea, coffee, wine and beer may decrease the risk).
[44] While supersaturation of urine may lead to crystalluria, it does not necessarily promote the formation of a kidney stone because the particle may not reach the sufficient size needed for renal attachment.
[48] In addition to Randall's plugs, which form in the Duct of Bellini, these structures can generate reactive oxygen species that further enhance stone formation.
Additionally, non-urease producing bacteria can provide bacterial components that promote calcium oxalate crystallization, though this mechanism is poorly understood.
[57] Calcium-containing stones are relatively radiodense (opaque to X-rays), and they can often be detected by a traditional radiography of the abdomen that includes the kidneys, ureters, and bladder (KUB film[clarification needed]).
Infection stones can grow rapidly, forming large calyceal staghorn (antler-shaped) calculi requiring invasive surgery such as percutaneous nephrolithotomy for definitive treatment.
In those with calcium stones, drinking plenty of fluids, thiazide diuretics and citrate are effective as is allopurinol in those with high uric acid levels in urine.
[90] Aside from vigorous oral hydration and eating more dietary calcium, other prevention strategies include avoidance of higher doses of supplemental vitamin C (since ascorbate is metabolized to oxalate) and restriction of oxalate-rich foods such as leaf vegetables, rhubarb, soy products and chocolate.
[101] Aside from alkalinization of the urine, these supplements have the added advantage of increasing the urinary citrate level, which helps to reduce the aggregation of calcium oxalate stones.
[85] Assuming no high-grade obstruction or associated infection is found in the urinary tract, and symptoms are relatively mild, various nonsurgical measures can be used to encourage the passage of a stone.
ESWL involves the use of a lithotriptor machine to deliver externally applied, focused, high-intensity pulses of ultrasonic energy to cause fragmentation of a stone over a period of around 30–60 minutes.
[108] Common adverse effects of ESWL include acute trauma, such as bruising at the site of shock administration, and damage to blood vessels of the kidney.
[111][112] In fact, the vast majority of people who are treated with a typical dose of shock waves using currently accepted treatment settings are likely to experience some degree of acute kidney injury.
[108] ESWL-induced acute kidney injury is dose-dependent (increases with the total number of shock waves administered and with the power setting of the lithotriptor) and can be severe,[108] including internal bleeding and subcapsular hematomas.
[108] To address these concerns, the American Urological Association established the Shock Wave Lithotripsy Task Force to provide an expert opinion on the safety and risk-benefit ratio of ESWL.
[108] The advantages of ESWL include its noninvasive nature, the fact that it is technically easy to treat most upper urinary tract calculi, and that, at least acutely, it is a well-tolerated, low-morbidity treatment for the vast majority of people.
[114] Beginning in the mid-1980s, less invasive treatments such as extracorporeal shock wave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy began to replace open surgery as the modalities of choice for the surgical management of urolithiasis.
The presence of indwelling ureteral stents may cause minimal to moderate discomfort, frequency or urgency incontinence, and infection, which in general resolves on removal.
[116] Research is currently uncertain if placing a temporary stent during ureteroscopy leads to different outcomes than not placing a stent in terms of number of hospital visits for post operative problems, short or long term pain, need for narcotic pain medication, risk of UTI, need for a repeat procedure or narrowing of the ureter from scarring.
[118] Ureteroscopic techniques are generally more effective than ESWL for treating stones located in the lower ureter, with success rates of 93–100% using Ho:YAG laser lithotripsy.
The Roman medical treatise De Medicina by Aulus Cornelius Celsus contained a description of lithotomy,[124] and this work served as the basis for this procedure until the 18th century.
[125] Examples of people who had kidney stone disease include Napoleon I, Epicurus, Napoleon III, Peter the Great, Louis XIV, George IV, Oliver Cromwell, Lyndon B. Johnson, Benjamin Franklin, Michel de Montaigne, Francis Bacon, Isaac Newton, Samuel Pepys, William Harvey, Herman Boerhaave, and Antonio Scarpa.
For domestic ruminants, dietary cation: anion balance is sometimes adjusted to assure a slightly acidic urine pH, for prevention of calculus formation.
[148] Various surgical interventions, e.g. amputation of the urethral process at its base near the glans penis in male ruminants, perineal urethrostomy, or tube cystostomy may be considered for relief of obstructive urolithiasis.