Pericarditis
[8] Symptoms typically include sudden onset of sharp chest pain, which may also be felt in the shoulders, neck, or back.
[4][8] Other causes include bacterial infections such as tuberculosis, uremic pericarditis, heart attack, cancer, autoimmune disorders, and chest trauma.
[4][5] Diagnosis is based on the presence of chest pain, a pericardial rub, specific electrocardiogram (ECG) changes, and fluid around the heart.
The pain is usually relieved by sitting up or bending forward, and worsened by lying down (both recumbent and supine positions) or by inspiration (taking a breath in).
[11] Other physical signs include a person in distress, positional chest pain, diaphoresis (excessive sweating); possibility of heart failure in form of pericardial tamponade causing pulsus paradoxus, and the Beck's triad of low blood pressure (due to decreased cardiac output), distant (muffled) heart sounds, and distension of the jugular vein (JVD).
A bedside electrocardiogram (ECG) shows widespread concave ST elevation and PR depression throughout most of the limb and precordial leads.
This can be seen in people who are experiencing the classic signs of pericarditis but then show signs of relief, and progress to show signs of cardiac tamponade which include decreased alertness and lethargy, pulsus paradoxus (decrease of at least 10 mmHg of the systolic blood pressure upon inspiration), low blood pressure (due to decreased cardiac index), (jugular vein distention from right sided heart failure and fluid overload), distant heart sounds on auscultation, and equilibration of all the diastolic blood pressures on cardiac catheterization due to the constriction of the pericardium by the fluid.
[citation needed] In such cases of cardiac tamponade, EKG or Holter monitor will then depict electrical alternans indicating wobbling of the heart in the fluid filled pericardium, and the capillary refill might decrease, as well as severe vascular collapse and altered mental status due to hypoperfusion of body organs by a heart that can not pump out blood effectively.
[citation needed] The diagnosis of tamponade can be confirmed with trans-thoracic echocardiography (TTE), which should show a large pericardial effusion and diastolic collapse of the right ventricle and right atrium.
[citation needed] The preferred initial diagnostic testing is the ECG, which may demonstrate a 12-lead electrocardiogram with diffuse, non-specific, concave ("saddle-shaped"), ST-segment elevations in all leads except aVR and V1[11] and PR-segment depression possible in any lead except aVR;[11] sinus tachycardia, and low-voltage QRS complexes can also be seen if there is subsymptomatic levels of pericardial effusion.
The following is the clinical classification of acute vs. chronic:[citation needed] The treatment in viral or idiopathic pericarditis is with aspirin,[11] or non-steroidal anti-inflammatory drugs (NSAIDs such as ibuprofen).
In this case, the patient is experiencing post-myocardial infarction pericarditis (PIP), which is characterized by chest pain, low-grade fever, and specific findings on physical examination and electrocardiogram.
[25][27][28][29] Surgical removal of the pericardium, pericardiectomy, may be used in severe cases and where the pericarditis is causing constriction, impairing cardiac function.
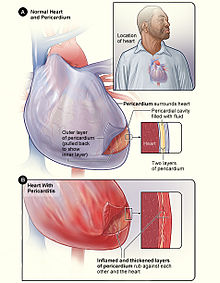
Figure B shows the heart with pericarditis. The inset image is an enlarged cross-section that shows the inflamed and thickened layers of the pericardium. [ 12 ]

