Second-degree atrioventricular block
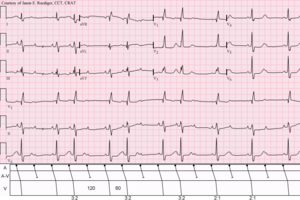
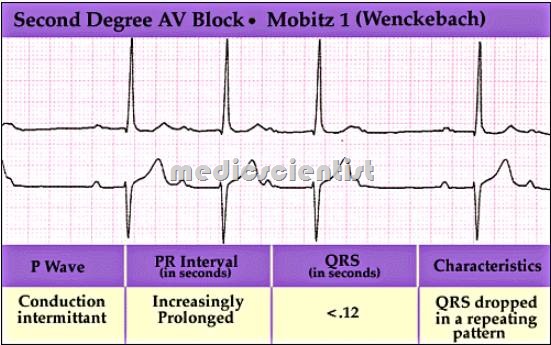
In Wenckebach's 1906 paper, his original observations were of increasing delay in contraction of the atria and ventricles that shortened after a brief pause.
After the dropped QRS complex, the PR interval resets and the cycle repeats.
[14] One of the baseline assumptions when determining if an individual has Mobitz I heart block is that the atrial rhythm has to be regular.
If the atrial rhythm is not regular, there could be alternative explanations as to why certain P waves do not conduct to the ventricles.
In symptomatic cases, intravenous atropine or isoproterenol may transiently improve conduction.
There is usually a fixed number of non-conducted P waves for every successfully conducted QRS complex, and this ratio is often specified in describing Mobitz II blocks.
[16]:179 This ratio is also frequently specified in referring to 3:1, 4:1, 5:1, or higher Mobitz type II block.
[citation needed] The P:QRS ratio is always of the form X:(X − 1) in type I Mobitz block.
[16]:182 In this case, a lengthened PR interval with a normal QRS width is most likely indicative of a type I-like pathology, and a normal PR interval with a widened QRS is most likely indicative of a type II-like pathology.

{kind=link}