Antinuclear antibody
They are found in many disorders including autoimmunity, cancer and infection, with different prevalences of antibodies depending on the condition.
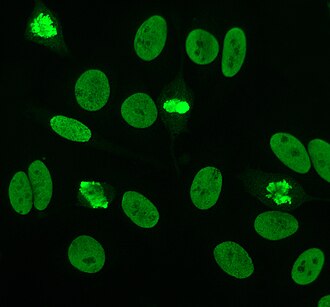
The common tests used for detecting and quantifying ANAs are indirect immunofluorescence and enzyme-linked immunosorbent assay (ELISA).
Although positive titres of 1:160 or higher are strongly associated with autoimmune disorders, they are also found in 5% of healthy individuals.
[9][10] Autoantibody screening is useful in the diagnosis of autoimmune disorders and monitoring levels helps to predict the progression of disease.
[8][11][12] A positive ANA test is seldom useful if other clinical or laboratory data supporting a diagnosis are not present.
In normal physiology, lymphocytes that recognise human proteins (autoantigens) either undergo programmed cell death (apoptosis) or become non-functional.
These disorders include: systemic lupus erythematosus (SLE), rheumatoid arthritis, Sjögren syndrome, scleroderma, polymyositis, dermatomyositis, primary biliary cirrhosis, drug induced lupus, autoimmune hepatitis, multiple sclerosis, discoid lupus, thyroid disease, antiphospholipid syndrome, juvenile idiopathic arthritis, psoriatic arthritis, juvenile dermatomyositis, idiopathic thrombocytopaenic purpura, infection and cancer.
[8][14] Extractable nuclear antigens (ENA) are a group of autoantigens that were originally identified as antibody targets in people with autoimmune disorders.
[16] Anti-Ro and anti-La antibodies, also known as SS-A and SS-B, respectively, are commonly found in primary Sjögren's syndrome, an autoimmune disorder that affects the exocrine glands.
[19][20] During pregnancy, anti-Ro antibodies can cross the placenta and cause heart block[21][22] and neonatal lupus in babies.
The La antigen is a 48kDa transcription termination factor of RNA polymerase III, which associates with the Ro-RNP complex.
[16][17][24][25] The mechanism of antibody production in Sjögren's syndrome is not fully understood, but apoptosis (programmed cell death) and molecular mimicry may play a role.
This may occur with one of the antigens, Ro or La, and may subsequently produce antibodies to other proteins through a process known as epitope spreading.
[26][30] The immune response to RNP may be caused by the presentation of the nuclear components on the cell membrane in apoptotic blebs.
Around 20–40% of polymyositis is positive for Jo-1 antibodies and most will have interstitial lung disease, HLA-DR3 and HLA-DRw52 human leukocyte antigen (HLA) markers; collectively known as Jo-1 syndrome.
Some anti-dsDNA antibodies are cross reactive with other antigens found on the glomerular basement membrane (GBM) of the kidney, such as heparan sulphate, collagen IV, fibronectin and laminin.
It is important to note that not all anti-dsDNA antibodies are associated with lupus nephritis and that other factors can cause this symptom in their absence.
[42][43] Anti-centromere antibodies are associated with limited cutaneous systemic sclerosis, also known as CREST syndrome, primary biliary cirrhosis and proximal scleroderma.
The sp100 antigen is found within nuclear bodies; large protein complexes in the nucleus that may have a role in cell growth and differentiation.
[48] Anti-DFS70 antibodies generate a dense fine speckled pattern in indirect immunofluorescence and are found in normals and in various conditions, but are not associated with a systemic autoimmune pathology.
A significant number of patients are diagnosed as systemic lupus erythematosus or undifferentiated connective tissue disease largely based on a positive ANA.
Higher titres are more clinically significant as low positives (≤1:160) are found in up to 20% of healthy individuals, especially the elderly.
Nuclear membrane staining appears as a fluorescent ring around the cell nucleus and are produced by anti-gp210 and anti-p62 antibodies.
[26][53][57][58] Indirect immunofluorescence has been shown to be slightly superior compared to ELISA in detection of ANA from HEp-2 cells.
They possess an organelle known as the kinetoplast which is a large mitochondrion with a network of interlocking circular dsDNA molecules.
The lack of other nuclear antigens in this organelle means that using C. luciliae as a substrate allows for the specific detection of anti-dsDNA antibodies.
[8][59][60] Enzyme-linked immunosorbent assay (ELISA) uses antigen-coated microtitre plates for the detection of ANAs.
The enzyme reaction will produce a change in colour of the solution that is proportional to the amount of antibody bound to the antigen.
For example, IgM-rheumatoid factor (IgM-RF) have been shown to cross-react with ANA giving falsely positive immunofluorescence.
[64] Positive ANA as well as anti-DNA antibodies have been reported in patients with autoimmune thyroid disease.