Aortic dissection
[3] In most cases, this is associated with a sudden onset of agonizing chest or back pain, often described as "tearing" in character.
[2] Aortic dissection can quickly lead to death from insufficient blood flow to the heart or complete rupture of the aorta.
[2][3] Major trauma, smoking, cocaine use, pregnancy, a thoracic aortic aneurysm, inflammation of arteries, and abnormal lipid levels are also associated with an increased risk.
[1][2] The diagnosis is suspected based on symptoms with medical imaging, such as CT scan, MRI, or ultrasound used to confirm and further evaluate the dissection.
[1] Dissections that involve the second part of the aorta can typically be treated with medications that lower blood pressure and heart rate, unless there are complications which then require surgical correction.
Less common symptoms that may be seen in the setting of AD include congestive heart failure (7%), fainting (9%), stroke (6%), ischemic peripheral neuropathy, paraplegia, and cardiac arrest.
Neurological complications of aortic dissection, such as stroke and paralysis, are due to the involvement of one or more arteries supplying portions of the central nervous system.
Proximal AD tends to be associated with weakening of the vascular wall due to cystic medial degeneration.
If the myocardial infarction is treated with thrombolytic therapy, the mortality increases to over 70%, mostly due to bleeding into the pericardial sac, causing cardiac tamponade.
The initial tear is usually within 100 mm of the aortic valve, so a retrograde dissection can easily compromise the pericardium leading to a hemopericardium.
[citation needed] While it is not always clear why an intimal tear may occur, quite often it involves degeneration of the collagen and elastin that make up the media.
Common tests used to diagnose an aortic dissection include a CT scan of the chest with iodinated contrast material and a transesophageal echocardiogram.
A level less than 500 ng/ml may be considered evidence against a diagnosis of aortic dissection,[1][31] although this guideline is only applicable in cases deemed "low risk"[32] and within 24 hours of symptom onset.
If there is high clinical suspicion, a more sensitive imaging test (CT angiogram, MR angiography, or transesophageal echo) may be warranted.
[citation needed] Computed tomography angiography is a fast, non-invasive test that gives an accurate three-dimensional view of the aorta.
To delineate the aorta to the accuracy necessary to make the proper diagnosis, an iodinated contrast material is injected into a peripheral vein.
[citation needed] Magnetic resonance imaging (MRI) is also used for the detection and assessment of aortic dissection, with a sensitivity of 98% and a specificity of 98%.
[citation needed] The transesophageal echocardiogram (TEE) is a good test in the diagnosis of aortic dissection, with a sensitivity up to 98% and a specificity up to 97%.
It is especially good in the evaluation of AI in the setting of ascending aortic dissection and to determine whether the ostia (origins) of the coronary arteries are involved.
However, type B dissections are not improved, from a mortality point of view, by the operation, unless leaking, rupture, or compromise to other organs, e.g. kidneys, occurs.
Repair may be recommended when greater than 4.5 cm (1.8 in) in size if the person has one of the several connective-tissue disorders or a family history of a ruptured aorta.
[42] Complicated Stanford type B aortic dissections require surgical intervention after initiation of medical therapy, with endovascular stent-grafting (TEVAR) available as a less invasive alternative to surgery.
[citation needed] Aortic dissection generally presents as a hypertensive emergency, and the prime consideration of medical management is to decrease the shear stress in the aortic wall (dP/dt (force of ejection of blood from the left ventricle)) by decreasing blood pressure and the heart rate.
In acute dissection, fast-acting agents can be given intravenously and have doses that are easier to adjust (such as esmolol, propranolol, or labetalol) is preferred.
Vasodilators such as sodium nitroprusside can be considered for people with ongoing high blood pressure, but they should never be used alone, as they often stimulate a reflexive increase in the heart rate.
[citation needed] Calcium channel blockers can be used in the treatment of aortic dissection, particularly if a contraindication to the use of beta-blockers exists.
Some treatments are:[citation needed] A number of comorbid conditions increase the surgical risk of repair of an aortic dissection.
[45] Establishing the incidence of aortic dissection has been difficult because many cases are only diagnosed after death (which may have been attributed to another cause), and is often initially misdiagnosed.
[25] In females before the age of 40, half of all aortic dissections occur during pregnancy (typically in the third trimester or early postpartum period).
[50] Surgery for aortic dissection was first introduced and developed by Michael E. DeBakey, Denton Cooley, and Oscar Creech, cardiac surgeons associated with the Baylor College of Medicine, Houston, Texas, in 1954.



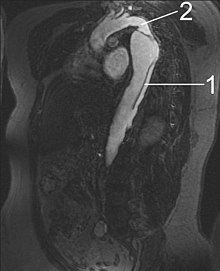
- Aorta descendens with dissection
- Aorta isthmus
