Hyperlipidemia
Hyperlipidemia is abnormally high levels of any or all lipids (e.g. fats, triglycerides, cholesterol, phospholipids) or lipoproteins in the blood.
Hyperlipidemia is usually chronic and requires ongoing medication to control blood lipid levels.
[4] The lipoprotein density and type of apolipoproteins it contains determines the fate of the particle and its influence on metabolism.
Lipid and lipoprotein abnormalities are common in the general population and are regarded as modifiable risk factors for cardiovascular disease due to their influence on atherosclerosis.
However, it can predispose one to more serious medical problems via lipid buildup, such as atherosclerosis (blood vessels), heart attack, or stroke (brain).
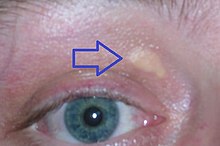
[6] Some indicators of hyperlipidemia are xanthomas, which are yellow "bumps" on the arms, legs, or trunk, or xanthelasmas, which are yellowish deposits of fat on the eyelids.
Smoking damages blood vessels, contributing to atherosclerosis and lowers HDL (good cholesterol) levels.
[11] Familial hyperlipidemias are classified according to the Fredrickson classification, which is based on the pattern of lipoproteins on electrophoresis or ultracentrifugation.
Complications include retinal vein occlusion, acute pancreatitis, steatosis, and organomegaly, and lipemia retinalis.
These individuals may present with a unique set of physical characteristics such as xanthelasmas (yellow deposits of fat underneath the skin often presenting in the nasal portion of the eye), tendon and tuberous xanthomas, arcus juvenilis (the graying of the eye often characterized in older individuals), arterial bruits, claudication, and of course atherosclerosis.
[24] The high VLDL levels are due to overproduction of substrates, including triglycerides, acetyl-CoA, and an increase in B-100 synthesis.
Also known as broad beta disease or dysbetalipoproteinemia, the most common cause for this form is the presence of ApoE E2/E2 genotype.
The receptor defect causes levels of chylomicron remnants and IDL to be higher than normal in the blood stream.
[31] In medicine, combined hyperlipidemia (or -aemia) (also known as "multiple-type hyperlipoproteinemia") is a commonly occurring form of hypercholesterolemia (elevated cholesterol levels) characterized by increased LDL and triglyceride concentrations, often accompanied by decreased HDL.
[33] Both conditions are treated with fibrate drugs, which act on the peroxisome proliferator-activated receptors (PPARs), specifically PPARα, to decrease free fatty acid production.
[9] They may result in increased risk of premature atherosclerosis or, when associated with marked hypertriglyceridemia, may lead to pancreatitis and other complications of the chylomicronemia syndrome.
A total cholesterol of higher than 240 mg/dL is abnormal, but medical intervention is determined by the breakdown of LDL and HDL levels.
[44] It can be affected by acquired or genetic factors, including tobacco use, obesity, inactivity, hypertriglyceridemia, diabetes, high carbohydrate diet, medication side effects (beta-blockers, androgenic steroids, corticosteroids, progestogens, thiazide diuretics, retinoic acid derivatives, oral estrogens, etc.)
[49][50] NCE-ATP III recommends all adults older than 20 to be screened as it may lead potential lifestyle modification that can reduce risks of other diseases.
[50] Management of hyperlipidemia includes maintenance of a normal body weight, increased physical activity, and decreased consumption of refined carbohydrates and simple sugars.
[52] Prescription drugs may be used to treat some people having significant risk factors,[52] such as cardiovascular disease, LDL cholesterol greater than 190 mg/dL or diabetes.
This was created by the National Heart, Lung, and Blood Institute in 1985 and combines physical activity, diet, and weight management to help lower cholesterol levels.
[54] Competitive inhibitors of HMG-CoA reductase, such as lovastatin, atorvastatin, fluvastatin, pravastatin, simvastatin, rosuvastatin, and pitavastatin, inhibit the synthesis of mevalonate, a precursor molecule to cholesterol.
[55] Fibric acid derivatives, such as gemfibrozil and fenofibrate, function by increasing the lipolysis in adipose tissue via activation of peroxisome proliferator-activated receptor-α.
[55] Major side effects include rashes, GI upset, myopathy, or increased transaminases.
[55] PCSK9 inhibitors are a newer drug class, approved by the FDA in 2015, which inhibit the liver-made enzyme (PCSK9), which typically breaks down LDL receptors.
[61][62] Over time fatty deposits can build up, hardening and narrowing the arteries until organs and tissues don't receive enough blood to properly function.
[42] Quitting smoking, lowering intake of saturated fat and alcohol, losing excess body weight, and eating a low-salt diet that emphasizes fruits, vegetables, and whole grains can help reduce blood cholesterol.