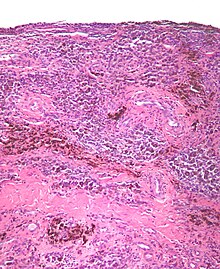
Tenosynovial giant cell tumor
[5] Diffuse TGCT (D-TGCT) — also called pigmented villonodular synovitis (PVNS)— is a rare tumor that presents as a proliferative, destructive, intra-articular lesion, most commonly in the knee.
[3]: 102 [6] Common symptoms of TGCT include swelling, pain, stiffness and reduced mobility in the affected joint or limb.
[3]: 100 [7]: 361 Localized and diffuse subsets of TGCT differ in their prognosis, clinical presentation, and biological behavior, but share a similar manner of disease development.
[3]: 100 [4]: 245 Localized TGCT tumors are typically 0.5 cm-4 cm),[3]: 101 develop over years,[3]: 100 are benign and non-destructive to the surrounding tissue, and may reoccur in the affected area.
[2]: 1 [7]: 361 [9]: 1 [3]: 102 Diffuse TGCT occurs less frequently and is locally aggressive (in some cases, tumors may infiltrate surrounding soft tissue).
If not treated early, it can spread to areas outside the joint, extra-articular, and potentially cause permanent loss of range as well as intense pain.
[24] Patients affected by TGCT should be managed within expert centers or reference networks, by a dedicated, experienced sarcoma multidisciplinary treatment team, including a pathologist, radiologist, orthopaedic surgeon, pain specialist, surgical, radiation and medical oncologists.
[28][29] There is insufficient and contradictory evidence on radiation therapy, in the form of radiosynoviorthesis (yttrium injections) or external beam, before or after surgery and thus no recommendation for its use in TGCT can be made.
[30][24] Active surveillance includes monitoring with MRI in intervals (e.g., every 6 months) to ensure the delay in treatment does not pose a potential harm.