Vascular access
Vascular access refers to a rapid, direct method of introducing or removing devices or chemicals from the bloodstream.
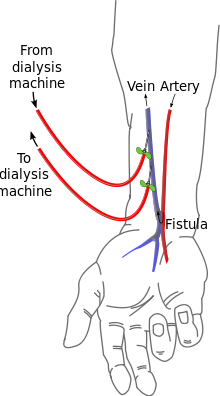
Three primary methods are used to gain access to the blood: an intravenous catheter, an arteriovenous fistula (AV) or a synthetic graft.
Catheter access is often popular with patients, because attachment to the dialysis machine doesn't require needles.
Placement in the groin is usually done when options in the arm and hands are not available due to anatomy or the failure of fistulas previously created in the arms/hands.
This sequence prevents partial recycling of the same blood through the dialysis machine, which would lead to less effective treatment.
One long-term complication of an AV fistula can be the development of an aneurysm, a bulging in the wall of the vein where it is weakened by the repeated insertion of needles over time.
To a large extent the risk of developing an aneurysm can be reduced by carefully rotating needle sites over the entire fistula ("rope-laddering"[3]), or using the "buttonhole" (constant site) technique; button-holing is safe when a fistula is used, but runs the risk of infection or degradation of an arterio-venous graft.
Fistulas can also become blocked due to blood clotting or infected if sterile precautions are not followed during needle insertion at the start of dialysis.
If that pressure is removed prematurely or a patient engages in physical activity too soon after dialysis, the needle holes can open up.
To prevent damage to the fistula and aneurysm or pseudoaneurysm formation, it is recommended that the needle be inserted at different points in a rotating fashion.
A recent study that was published in The American Journal of Pathology, provides information about the mechanisms underlying failure of the most common type of hemodialysis vascular access, the arteriovenous fistula.
This research raises the possibility that therapeutic restoration of nitric oxide responsiveness through manipulation of local mediators may prevent fistula maturation failure in patients and potentially contribute to their ability to remain on hemodialysis.
[4] AV (arteriovenous) grafts are much like fistulas in most respects, except that an artificial vessel is used to join the artery and vein.
They mature faster than fistulas, and may be ready for use several weeks after formation (some newer grafts may be used even sooner).