Transjugular intrahepatic portosystemic shunt
An interventional radiologist creates the shunt using an image-guided endovascular (via the blood vessels) approach, with the jugular vein as the usual entry site.
It was first used in a human patient by Dr. Ronald Colapinto, of the University of Toronto, in 1982, but did not become reproducibly successful until the development of endovascular stents in 1985.
[1] The procedure has since become widely accepted as the preferred method for treating portal hypertension that is refractory to medical therapy, replacing the surgical portacaval shunt in that role.
On the other hand, up to 25% of patients who undergo TIPS will experience transient post-operative hepatic encephalopathy caused by increased porto-systemic passage of nitrogen from the gut.
Thus, in people with advanced liver disease the shunting of portal blood away from hepatocytes is usually well tolerated.
[7] Lastly, the TIPS may become blocked by a blood clot or in-growth of endothelial cells and no longer function.
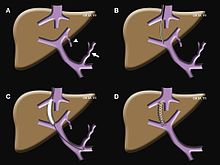
[citation needed] A TIPS procedure decreases the effective vascular resistance of the liver through the creation of an alternative pathway for portal venous circulation.
[citation needed] Transjugular intrahepatic portosystemic shunts are typically placed by an interventional radiologist under fluoroscopic guidance.
Once access to the jugular vein is confirmed, a guidewire and introducer sheath are typically placed to facilitate the shunt's placement.