Magnetic resonance angiography
The most frequently applied MRA methods involve the use intravenous contrast agents, particularly those containing gadolinium to shorten the T1 of blood to about 250 ms, shorter than the T1 of all other tissues (except fat).
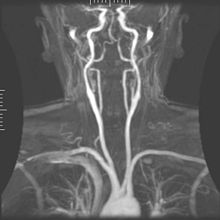
It is also the most common technique used for routine angiographic evaluation of the intracranial circulation in patients with ischemic stroke.
[1] Phase-contrast (PC-MRA) can be used to encode the velocity of moving blood in the magnetic resonance signal's phase.
[3] The most common method used to encode velocity is the application of a bipolar gradient between the excitation pulse and the readout.
, is null: The bipolar gradient can be applied along any axis or combination of axes depending on the direction along which flow is to be measured (e.g.
, of the MRI signal is manipulated by bipolar gradients (varying magnetic fields) that are preset to a maximum expected flow velocity.
One of the main advantages of this kind of techniques is that we may image the regions of slow flow often found in patients with vascular diseases more easily.
Contrast-enhanced magnetic resonance angiography uses injection of MRI contrast agents and is currently the most common method of performing MRA.
[2][6] The contrast medium is injected into a vein, and images are acquired both pre-contrast and during the first pass of the agent through the arteries.
By subtraction of these two acquisitions in post-processing, an image is obtained which in principle only shows blood vessels, and not the surrounding tissue.
A problem, however, is the fact that both arteries and veins are enhanced at the same time if higher resolution images are required.
An important condition for this approach is to have excellent body fat suppression over large image areas, which is possible by using mDIXON acquisition methods.
mDIXON methods can distinguish and accurately separate image signals created by fat or water.
By using the 'water images' for MRA scans, virtually no body fat is seen so that no subtraction masks are needed for high quality MR venograms.
A notable non-enhanced method for flow-independent angiography is balanced steady-state free precession (bSSFP) imaging which naturally produces high signal from arteries and veins.
To avoid these complications as well as eliminate the costs of contrast media, non-enhanced methods have been researched recently.
Flow-independent NEMRA methods are not based on flow, but exploit differences in T1, T2 and chemical shift to distinguish blood from static tissue.
Trade names for this technique include Fresh Blood Imaging (Toshiba), TRANCE (Philips), native SPACE (Siemens) and DeltaFlow (GE).
This method is based on the different signal properties of blood compared to other tissues in the body, independent of MR flow effects.
MRA techniques in general are sensitive to turbulent flow, which causes a variety of different magnetized proton spins to lose phase coherence (intra-voxel dephasing phenomenon), resulting in a loss of signal.
The most common method is maximum intensity projection (MIP), where the computer simulates rays through the volume and selects the highest value for display on the screen.
If several such projections are combined into a cine loop or QuickTime VR object, the depth impression is improved, and the observer can get a good perception of 3D structure.
An alternative to MIP is direct volume rendering where the MR signal is translated to properties like brightness, opacity and color and then used in an optical model.
Most often, the underlying disease is atherosclerosis, but medical conditions like aneurysms or abnormal vascular anatomy can also be diagnosed.
It is also ruled out in patients for whom MRI exams may be unsafe (such as having a pacemaker or metal in the eyes or certain surgical clips).
MRA procedures for visualizing cranial circulation are no different from the positioning for a normal MRI brain.