Caffeine
Evidence of a risk during pregnancy is equivocal; some authorities recommend that pregnant women limit caffeine to the equivalent of two cups of coffee per day or less.
[45] It appears that caffeine in low doses improves airway function in people with asthma, increasing forced expiratory volume (FEV1) by 5% to 18% for up to four hours.
[9] At normal doses, caffeine has variable effects on learning and memory, but it generally improves reaction time, wakefulness, concentration, and motor coordination.
[71] For the general population of healthy adults, Health Canada advises a daily intake of no more than 400 mg.[72] This limit was found to be safe by a 2017 systematic review on caffeine toxicology.
[78] This recommendation is based on a clinical report released by American Academy of Pediatrics in 2011 with a review of 45 publications from 1994 to 2011 and includes inputs from various stakeholders (Pediatricians, Committee on nutrition, Canadian Pediatric Society, Centers for Disease Control & Prevention, Food and Drug Administration, Sports Medicine & Fitness committee, National Federations of High School Associations).
[78] For children age 12 and under, Health Canada recommends a maximum daily caffeine intake of no more than 2.5 milligrams per kilogram of body weight.
Based on average body weights of children, this translates to the following age-based intake limits:[72] Health Canada has not developed advice for adolescents because of insufficient data.
[81] A 2011 review found that caffeine during pregnancy does not appear to increase the risk of congenital malformations, miscarriage or growth retardation even when consumed in moderate to high amounts.
[84] A systematic review, analyzing the results of observational studies, suggests that women who consume large amounts of caffeine (greater than 300 mg/day) prior to becoming pregnant may have a higher risk of experiencing pregnancy loss.
[94][95][96] Minor undesired symptoms from caffeine ingestion not sufficiently severe to warrant a psychiatric diagnosis are common and include mild anxiety, jitteriness, insomnia, increased sleep latency, and reduced coordination.
The frequency at which this occurs is self-reported at 11%, but in lab tests only half of the people who report withdrawal actually experience it, casting doubt on many claims of dependence.
[121][124] The APA, which published the DSM-5, acknowledged that there was sufficient evidence in order to create a diagnostic model of caffeine dependence for the DSM-5, but they noted that the clinical significance of the disorder is unclear.
[140][145][146] Intralipid infusion therapy is indicated in cases of imminent risk of cardiac arrest in order to scavenge the free serum caffeine.
The fatal dose in humans is estimated to be 150–200 milligrams per kilogram, which is 10.5–14 grams for a typical 70 kg (150 lb) adult, equivalent to about 75–100 cups of coffee.
[177] As a competitive nonselective phosphodiesterase inhibitor,[178] caffeine raises intracellular cyclic AMP, activates protein kinase A, inhibits TNF-alpha[179][180] and leukotriene[181] synthesis, and reduces inflammation and innate immunity.
[5] The half-life is decreased by 30-50% in adult male smokers, approximately doubled in women taking oral contraceptives, and prolonged in the last trimester of pregnancy.
[196] This is presumably due to the need for a higher intake to achieve a comparable desired effect, not that the gene led to a disposition for greater incentive of habituation.
[214] Caffeine can be quantified in blood, plasma, or serum to monitor therapy in neonates, confirm a diagnosis of poisoning, or facilitate a medicolegal death investigation.
Plasma caffeine levels are usually in the range of 2–10 mg/L in coffee drinkers, 12–36 mg/L in neonates receiving treatment for apnea, and 40–400 mg/L in victims of acute overdosage.
Urinary caffeine concentration is frequently measured in competitive sports programs, for which a level in excess of 15 mg/L is usually considered to represent abuse.
[224] Caffeine in nectar may improve the reproductive success of the pollen producing plants by enhancing the reward memory of pollinators such as honey bees.
[249] Tablets offer several advantages over coffee, tea, and other caffeinated beverages, including convenience, known dosage, and avoidance of concomitant intake of sugar, acids, and fluids.
[266] The leaves and stems of the yaupon holly (Ilex vomitoria) were used by Native Americans to brew a tea called asi or the "black drink".
[267] In 1819, the German chemist Friedlieb Ferdinand Runge isolated relatively pure[vague] caffeine for the first time; he called it "Kaffebase" (i.e., a base that exists in coffee).
[272] However, Berzelius later acknowledged Runge's priority in the extraction of caffeine, stating:[273] "However, at this point, it should not remain unmentioned that Runge (in his Phytochemical Discoveries, 1820, pages 146–147) specified the same method and described caffeine under the name Caffeebase a year earlier than Robiquet, to whom the discovery of this substance is usually attributed, having made the first oral announcement about it at a meeting of the Pharmacy Society in Paris."
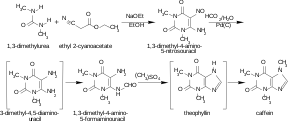
In 1895, German chemist Hermann Emil Fischer (1852–1919) first synthesized caffeine from its chemical components (i.e. a "total synthesis"), and two years later, he also derived the structural formula of the compound.
[295] The Seventh-day Adventist Church asked for its members to "abstain from caffeinated drinks", but has removed this from baptismal vows (while still recommending abstention as policy).
In the 16th century, some Muslim authorities made unsuccessful attempts to ban them as forbidden "intoxicating beverages" under Islamic dietary laws.
[306] Nachdem Goethe mir seine größte Zufriedenheit sowol über die Erzählung des durch scheinbaren schwarzen Staar Geretteten, wie auch über das andere ausgesprochen, übergab er mir noch eine Schachtel mit Kaffeebohnen, die ein Grieche ihm als etwas Vorzügliches gesandt.
Er hatte recht; denn bald darauf entdeckte ich darin das, wegen seines großen Stickstoffgehaltes so berühmt gewordene Coffein.Caffeine-induced increases in performance have been observed in aerobic as well as anaerobic sports (for reviews, see [26,30,31])...